NM 28 yrs olf female patient was presented for Diagnostic and Therapeutic Hystero Laparoscopy under General Anaesthesia for primary infertility and possible tubal block.
A preoperative evaluation revealed that she was having RBBB and Left Anerior hemiblock ( Bifacicular block). a 2D Echo cardiography by the cardiologist no other problem with Good LV function and a mild Diastolic dysfunction. She was healthy . Blood reports including Sodium and Pottasium was normal. Airway Normal, She was planned GA with LMA/iGEl intubation. with Scholine and Non depolarising muscle relaxant to be added if the procedure is prolonged





Her blood pressure was 140/90, Radial pulse was feeble but palpable. In the meantime surgical procedure was over CO2 removed . But the tachycardia continued. An injection of Ameodarone 150 mg started in a syringe pump as a loading dose. The heart rate came down to 160-170 / min with stable blood presuure. In the mean time the patient recovered from Anaesthesia . and we decided to shift to HDU and continue therapy and monitor the pt closely . Injection of Ameodarone loading dose had no effect. Thinking it might cause a precipitation of block the dose was reduced for sometime.Addition of some more Xylocard brought down Heart rate to 140 but reverted back to 160-170
By this time pt was fully awake and did not seem to have any discomfort or complain. We also consulted the Cardiologist who advised to continue Ameodarone therapy after the loading dose. So initially 30mg / hour follwoerd by 60 mg / hour. After one more hour the patient had a bout of vomiting and suddenly the heart rate dropped to 88 /min. and continued to remain so.,
Next a repeat ECG showed the same ECG pattern as it was before surgery.( picture)
The patient was discharged next day.
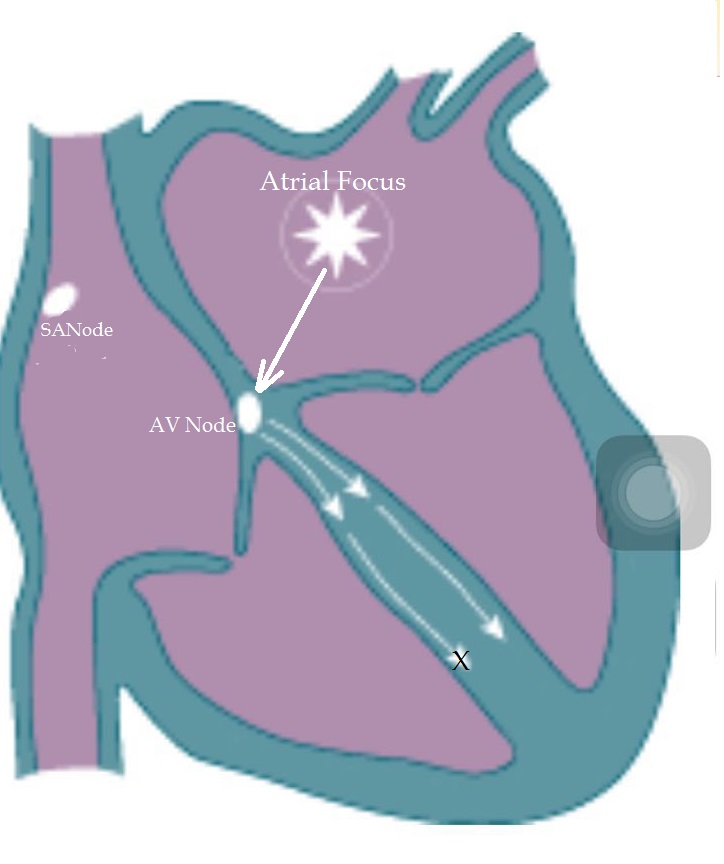

it is very difficult to comprehend why the rhythm was converted to a different kind . As you can see the picture above the atrial focus caused the pattern possibly.
There was no Hypoxia,or Acidosis, or electrolyte disturbance to make a dramatic change.
How ever Ameodarone remains the drug of choice and very effective.
No comments:
Post a Comment